End-Tidal CO2
What Is Capnography?
Capnography is the monitoring of the concentration or partial pressure of carbon dioxide (CO2) in respiratory gases.
End tidal CO2 (EtCO2) is the maximum expired carbon dioxide concentration during a respiratory cycle.
The graphical representation of EtCO2 is shown in a waveform format and is known as a capnogram.
A normal capnogram as displayed on the ZOLL R Series monitor/defibrillator.

CO2 monitoring provides information not only regarding pulmonary function, but also indirect cardiac function, ventilator function, and perfusion.
Download a pocket guide to common abnormal capnograms.
Why Use Capnography?
In the American Heart Association (AHA) 2015 Guidelines, continuous waveform capnography is a Class I, LOE A recommendation for confirming and monitoring correct placement of an endotracheal tube.1
Because a sustained increase in PETCO2 during CPR is an indicator of return of spontaneous circulation (ROSC), the AHA Guidelines also recommend using capnography in intubated patients to monitor CPR quality, optimize chest compressions, and detect ROSC during chest compressions or when the rhythm check reveals an organized rhythm (Class IIb, LOE C).1
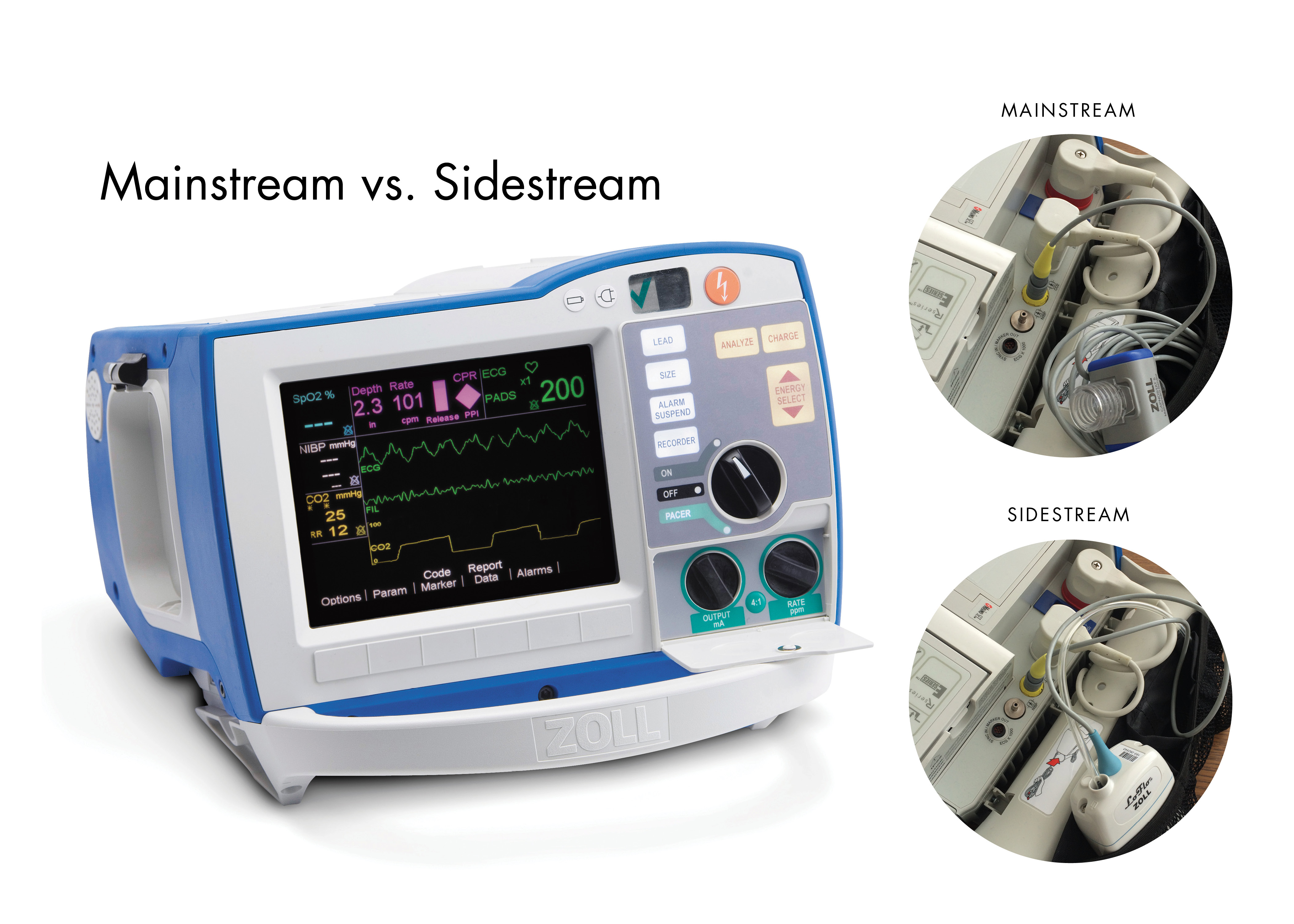
Mainstream and Sidestream Available on One Defibrillator
The R Series® is the only monitor/defibrillator that offers both mainstream and sidestream capnography. Depending on the needs of your patient, exchanging mainstream technology for sidestream is seamless. It’s as simple as unplugging one cable and exchanging it for another.
What Is Mainstream Capnography?
Mainstream capnography is most commonly used for mechanically ventilated patients and intubated patients who require intensive monitoring. Mainstream devices can also be used on non-intubated patients, but require a mouthpiece or a mask.
With mainstream capnography, the airway adapter is placed directly in the breathing circuit in between the ventilator “Y” and the elbow adapter, as shown in the diagram.

A mainstream sensor is then attached to the adapter. As the patient exhales, the CO2-rich gas passes through the airway adapter, where it is measured. Because the mainstream sensor is not in direct contact with the patient, it cannot be contaminated by moisture or secretions. If the mainstream airway adapter becomes contaminated with secretions, water, or by an aerosolized medication, it can be removed and replaced. The actual mainstream sensor does not need to be replaced.
Mainstream Capnography on the R Series

Benefits of mainstream capnography include:
- Rapid warm-up time allows you to start monitoring faster
- No clogging due to secretions
- No water traps or tubing needed
- Easy-to-use airway adapters provide hassle-free uninterrupted monitoring
- No calibration required
- Displays a printable capnogram on the defibrillator screen for easy identification of abnormal waveforms
Sidestream Capnography on the R Series
Sidestream measurement is aspirated through a nasal cannula via an internal sampling pump, the LoFlo® Sidestream System. Sidestream is ideal for non-intubated patients.

Benefits of sidestream capnography:
- IR sensor is located remote from the patient
- 50 ml/min sampling rate
- Can be used on intubated patients via an on-airway adapter kit
- Removable and disposable sample cell and filter protects the LoFlo from contamination
- Can be mounted on bedrail or pole
- 24,000 hour pump life
- No calibration required
- For use on all patient populations
- Full LoFlo accessory offering – adult to infant/neonates
- Displays a printable capnogram on the defibrillator screen for easy identification of abnormal waveforms
1Link MS, et al. “Part 7: Adult Advanced Cardiovascular Life Support. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.” Circulation. 2015; 132(suppl 2): S444–S464.